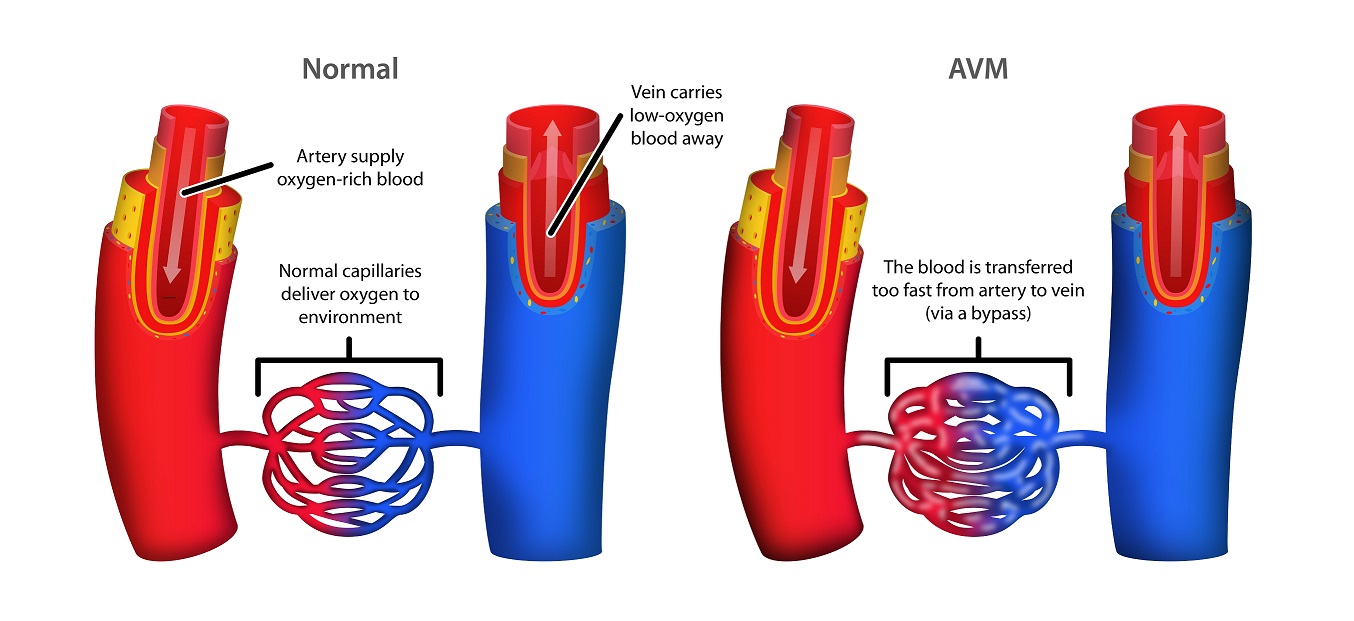
Arteriovenous malformations (AVMs) are abnormal connections between arteries and veins that are congenital (present at birth) but grow and expand with time. Normally the arteries and veins are connected by a network of tiny vessels called capillaries. These capillary beds provide an important function for the circulatory system by providing the site at which oxygen (carried in blood by the red blood cells) can be released into the muscles, fat, and other tissues where it is needed. When a direct artery-vein connection occurs (and the capillary bed is missing), normal oxygen exchange cannot occur, and the body senses a lack of oxygen (or hypoxia) in that area. This lack of oxygen creates the environment which ultimately causes an AVM to grow.
AVMs are relatively rare. They occur approximately once in every 500 births. This means that only 1-2 people per every 100,000 people has an AVM. AVMs in the brain are more common than AVMs elsewhere in the body.
What causes AVMs?
The cause of AVMs is unknown. They are believed to be caused by a mistake in the formation of the normal connections between arteries and veins (called capillaries) that occurs during early embryonic life. No known food, medication, or activity during pregnancy can cause an AVM.
We now know some AVMs are caused by genetic changes that are inherited or hereditary and some are caused by gene changes that are somatic or acquired
Some of the hereditary syndromes known to be associated with AVMs are:
Hereditary hemorrhagic telangiectasia (HHT) – A fairly common inherited vascular disorder. Children with HHT can develop AVMs in the lungs, brain, and gastrointestinal tract. Often associated with significant nosebleeds.
Capillary malformation-Arteriovenous malformation syndrome (CM-AVM) – Much less common than HHT. Can have similar symptoms but may have different skin findings or locations of AVMs.
Parkes-Weber syndrome – A disorder in which there are AVMs, overgrowth of a limb, and usually capillary malformations or port wine stains on the skin.
There are other very rare syndromes in which AVMs can form in the eye (Wyburn-Mason syndrome) or spinal cord (Cobb syndrome).
What are the symptoms of AVMs?
AVMs develop before birth but may not be apparent until later in life.
Sometimes an AVM can look just like an innocent birthmark on your child’s skin but can begin to enlarge and cause issues in childhood or adolescence.
Intracranial (within the head) AVMs have no visible symptoms. However, they may cause headaches or sudden bleeding into the brain.
AVMs outside the brain appear more slowly with color changes, swelling, and pain.
Some AVMs can also present with bleeding or may intermittently have bleeding.
If left untreated, some AVMs can cause extra strain on the heart which can lead to heart failure.
Sometimes a “heartbeat” or pulse may be felt within the AVM.
In time, if the blood flow through an AVM is excessive, your child’s heart can become overworked.
AVMs can occur in any organ in the body. They occur most frequently in the parts of the body below (in order of frequency):
Head.
Limbs.
Trunk.
Internal organs.
In infancy and childhood, the blush of an AVM can be mistaken for a hemangioma or other vascular malformation.
The AVM becomes obvious as signs of fast blood flow appear. The skin becomes a darker red or purple color, nearby veins enlarge, a mass appears beneath the stain, and there is local warmth. Sometimes you can feel a pulse over the AVM.
How is an AVM diagnosed?
Many AVMs can be diagnosed based on physical examination and medical history alone. However, many times your doctor will order an ultrasound, MRI (magnetic resonance imaging), and/or an angiogram (where a special dye is injected to evaluate the blood vessels in more detail. A procedure which involves traveling through the arteries to inject the vessels and better understand the makeup of the AVM.
What are Important Things to Know About AVMs?
Because AVMs are “high-flow” or “fast-flow” malformations, they can bleed significantly. An AVM should never be biopsied without great care and preparation.
If you have an AVM, you should talk to your doctor about the best treatment plan for your particular AVM. Sometimes this may include “watching and waiting” as sometimes procedures can lead to more complications.
Everyone diagnosed with an AVM should have a thorough family history review and some patients should have genetic testing.
How are AVMs treated?
Treatment usually depends on where your child’s AVM is located. It also depends on the symptoms associated with the AVM, the age of the child, and whether there are risks for development of new AVMs in the future.
Intracranial AVMs:
Radiation.
Embolization (injection of material into the center of the anomaly via a catheter).
Surgical resection.
AVMs in other parts of the body:
Embolization.
Sclerotherapy (direct injection of an irritating solution).
Surgery.
Medical therapy*.
Wherever possible, surgery or complete embolization provides the best treatment. However, many AVMs cannot be fully treated so the symptoms must be managed carefully over time.
*Researchers are working hard to find medicines to help treat AVMs, but these are currently considered experimental. Some experts in AVMs are testing drugs that inhibit blood vessel growth as well as drugs that inhibit the known genetic changes seen in AVMs.